Dr. Erick Kazarian, MD
NYU Langone Spine Surgery — Patient Information
Scan the QR code to view this page online →

Endoscopic Microdiscectomy/Laminectomy
Understanding Biportal Endoscopic Spine Surgery (BESS)
Biportal Endoscopic Spine Surgery (BESS) is a state-of-the-art minimally invasive technique used to relieve pressure on spinal nerves caused by herniated discs, bone spurs, or spinal stenosis. Unlike traditional open back surgery, BESS uses two small portals (incisions) — one for a high-definition endoscopic camera and one for surgical instruments — to access the problem area in the spine. This two-portal approach gives Dr. Kazarian exceptional visualization and freedom of movement, allowing precise removal of only the tissue that is compressing the nerve while preserving the surrounding healthy structures.
BESS is most commonly performed to treat lumbar (lower back) conditions such as herniated or bulging discs that cause sciatica, as well as spinal stenosis that narrows the spinal canal and puts pressure on nerve roots. During a microdiscectomy, the surgeon removes the portion of the disc that is pressing on a nerve. During a laminectomy, a small amount of bone (the lamina) is removed to create more space in the spinal canal. In many cases, both techniques are combined in a single procedure to achieve the best possible outcome for the patient.
The advantages of the biportal endoscopic approach include smaller incisions and minimal muscle damage, better visualization of the surgical field using the high-definition endoscopic camera, less postoperative pain compared to traditional open surgery, faster recovery and earlier return to normal activities, and a lower risk of infection and scarring. The goal of the procedure is to remove the portion of the disc or bone that is pressing on the nerve, relieving pain and restoring mobility. Most patients go home the same day and are able to return to light daily activities within one to two weeks.
Images & Diagrams
Pre-Operative Instructions
Careful preparation before your surgery helps ensure the safest possible experience and the best outcome. Please follow these instructions and contact our office if you have any questions.
Review all current medications and supplements with Dr. Kazarian.
1-2 weeks before surgeryStop blood thinners (warfarin, aspirin, Plavix), NSAIDs (ibuprofen, naproxen), and herbal supplements (fish oil, vitamin E, ginkgo) as directed. GLP-1 receptor agonists (Ozempic, Wegovy, Mounjaro, Trulicity, Saxenda) must be stopped 7 days before surgery due to the risk of aspiration under anesthesia. Do not stop any medication without Dr. Kazarian's approval.
Obtain medical clearance from your primary care physician and any relevant specialists.
2-4 weeks before surgeryThis may include blood work, an EKG, and a health review. Bring clearance letters and your CPAP machine (if applicable) on surgery day.
Do not eat or drink anything after midnight the night before surgery.
After midnight the night before surgeryThis includes water, coffee, gum, and mints. You may take approved medications with a small sip of water.
The NYU perioperative team will call you the day before surgery with your arrival time.
Day of surgeryLocation: NYU Langone Kimmel Pavilion, 424 East 34th Street, Manhattan. Bring a valid photo ID, insurance card, and medication list.
Arrange for a responsible adult to drive you home and stay with you for 24 hours.
Day of surgeryYou cannot drive after anesthesia. Your driver should stay at the hospital during the procedure.
What to Expect on Surgery Day
Biportal endoscopic spine surgery is typically an outpatient procedure, meaning you can expect to go home the same day. Here is an overview of what your experience will be like from arrival through discharge.
Check-In and Pre-Operative Preparation
When you arrive at the hospital, our team will greet you, confirm your identity and medical information, and review your consent forms. You will change into a hospital gown and have an IV line placed for fluids and medication. Your anesthesiologist will meet with you to discuss your anesthesia plan, and Dr. Kazarian will mark the surgical site and answer any remaining questions you may have.
Anesthesia and Positioning
You will be brought to the operating room and positioned comfortably on your stomach (prone position) on a specialized surgical table. General anesthesia is most commonly used, so you will be fully asleep and feel no pain throughout the procedure. In select cases, Dr. Kazarian may recommend sedation with local anesthesia. Once you are anesthetized, the surgical team will use fluoroscopic (live X-ray) imaging to precisely locate the affected level of your spine.
Two-Portal Incisions and Endoscope Insertion
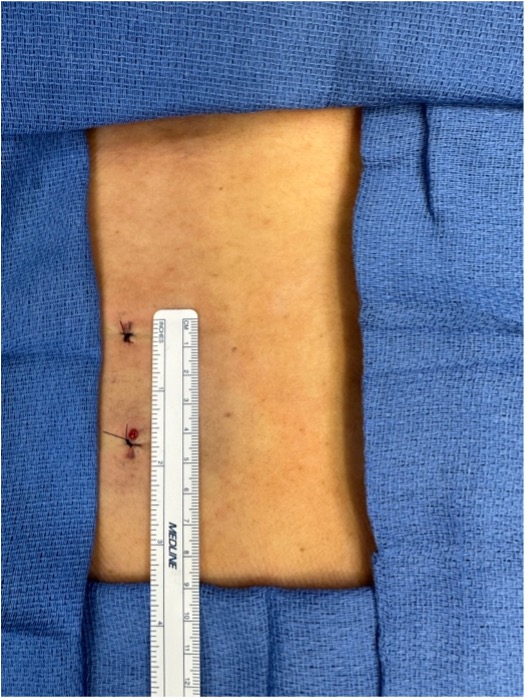
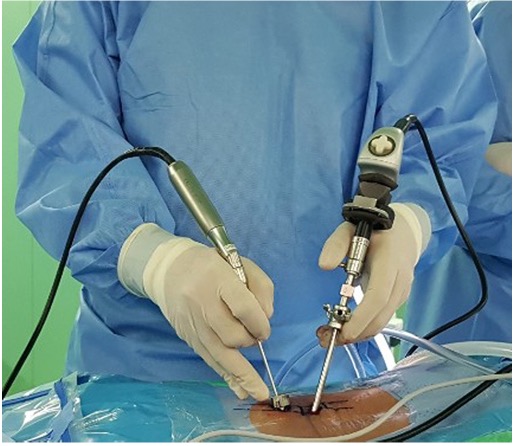
Dr. Kazarian makes two small incisions (portals), each approximately 7 to 10 millimeters, near the affected area of your spine. One portal is used for the high-definition endoscopic camera, and the other is used for the surgical instruments. The muscles are gently dilated apart rather than cut, which greatly reduces tissue damage. This biportal technique provides Dr. Kazarian with an excellent view of the surgical area and full freedom of instrument movement, allowing greater precision than a single-portal approach.
Nerve Decompression
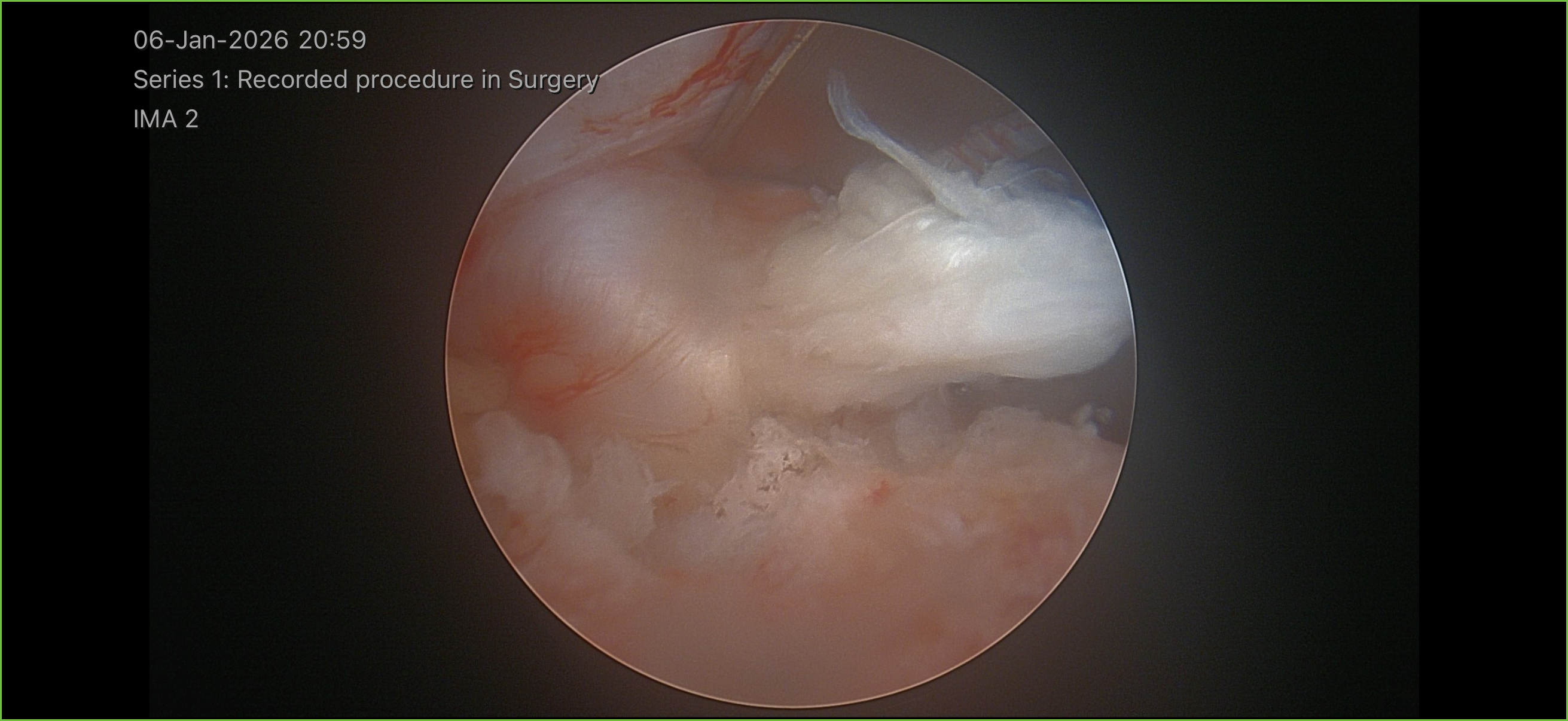
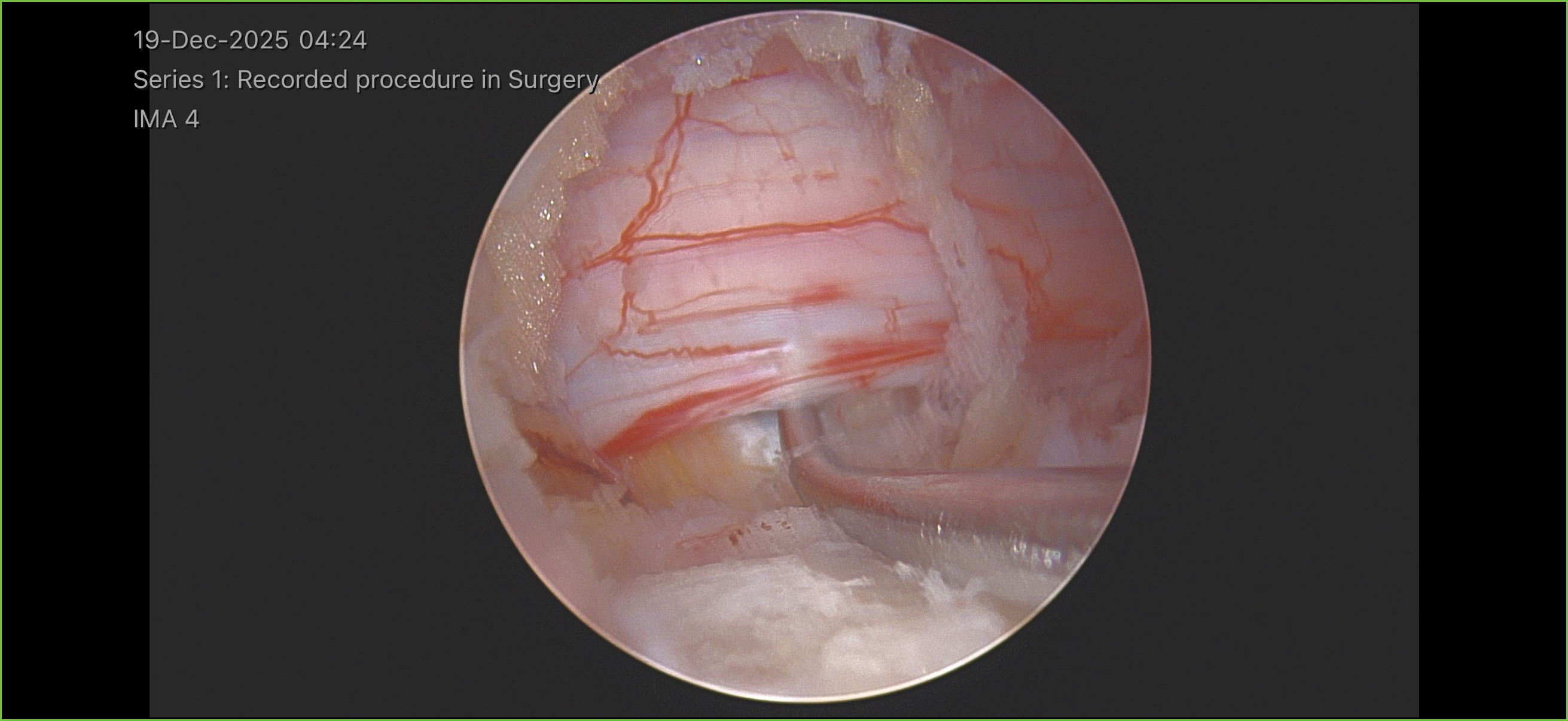
Using specialized micro-instruments through the instrument portal, Dr. Kazarian carefully removes the herniated disc fragment, bone spur, or thickened ligament that is compressing the spinal nerve while viewing the entire procedure through the camera portal. If a laminectomy is needed, a small portion of the lamina bone is precisely removed to widen the spinal canal. The high-definition endoscopic camera provides real-time visualization so Dr. Kazarian can protect the nerve root and surrounding structures with exceptional accuracy. The entire process typically takes 45 to 90 minutes.
Closure and Recovery Room
Once the nerve is fully decompressed, the endoscope and instruments are removed. The two small incisions are closed with a few stitches or adhesive strips and covered with sterile bandages. You will be taken to the recovery room, where our nursing team will monitor your vital signs, manage any discomfort, and help you begin moving safely. Most patients are able to stand and walk within one to two hours after surgery. Before discharge, your care team will review your pain management plan, activity guidelines, and follow-up appointment schedule with you and your companion.
Risks & Potential Complications
Biportal endoscopic spine surgery is a minimally invasive procedure with a strong safety profile. However, as with any surgery, there are potential risks and complications that you should be aware of. Dr. Kazarian will discuss these with you in detail during your consultation.
Infection
Any time an incision is made, there is a small risk of infection at the surgical site. Because the two portal incisions used in BESS are very small, the risk of infection is lower than with traditional open surgery. Signs of infection include increasing redness, swelling, warmth, or drainage from either incision, as well as fever.
Blood Loss
Some bleeding is expected during any surgery. Due to the minimally invasive nature of this procedure, blood loss is typically minimal. Significant blood loss requiring a transfusion is very rare.
Cerebrospinal Fluid (CSF) Leak
The spinal cord and nerves are surrounded by a protective membrane that contains cerebrospinal fluid. In rare cases, this membrane can be nicked during surgery, causing a fluid leak. If this occurs, it is typically repaired during the procedure and may require a short period of additional bed rest to allow it to heal.
Recurrent Disc Herniation
After a microdiscectomy, there is a chance that the same disc can herniate again in the future. This occurs in a small percentage of patients and may happen weeks, months, or even years after the original surgery. If a recurrent herniation causes significant symptoms, additional treatment or surgery may be needed.
Incomplete Resolution of Symptoms
While most patients experience significant relief from leg pain and sciatica after surgery, there is a possibility that some of your pre-operative symptoms may not fully resolve. This can happen if the nerve was compressed for an extended period before surgery or if there are other contributing factors to your pain. Dr. Kazarian will discuss realistic expectations with you based on your specific condition.
Neurologic Injury
Although uncommon, there is a risk of injury to the spinal nerves during surgery. This could result in new or worsened numbness, tingling, or weakness in one or both feet or legs. Dr. Kazarian uses magnification, specialized instruments, and careful technique to minimize this risk.
Recovery
Recovery from biportal endoscopic spine surgery is significantly faster than recovery from traditional open spine surgery — most patients measure their recovery in weeks, not months. Because the procedure uses two very small incisions and preserves the surrounding muscles and tissues, postoperative pain is generally mild and manageable. Many patients notice immediate relief of their leg pain (sciatica) upon waking from surgery, though some numbness or tingling may take longer to resolve. Following Dr. Kazarian's activity guidelines and attending all follow-up appointments are key to a smooth and successful recovery.
Prescribed Medications
| Medication | Type | Dosage | Frequency | When to Take |
|---|---|---|---|---|
| Flexeril (cyclobenzaprine) | Muscle Relaxer | 5 mg | Every 6 hours as needed | Take for moderate to severe muscle spasm or pain |
| Tylenol (acetaminophen) | Pain Reliever | 500–1000 mg | Every 6 hours as needed | Take for mild pain |
| Tramadol | Semi-Narcotic Pain Reliever | 75 mg | Every 6 hours as needed | Take for moderate to severe pain not controlled by Tylenol or NSAIDs |
Always take medications exactly as prescribed by your surgeon. Do not combine pain medications without consulting your doctor.
First Few Days After Surgery
You may go home the same day as your procedure or, in some cases, the following morning. It is normal to experience mild to moderate soreness at the incision site, and some patients notice immediate improvement in their leg pain or sciatica symptoms. You will be encouraged to walk short distances several times a day to promote circulation and healing. Dr. Kazarian will prescribe pain medication and a muscle relaxant if needed.
- No bending, twisting, or lifting anything heavier than 5 pounds
- No driving while taking prescription pain medication
- Avoid sitting for more than 20 to 30 minutes at a time
- Keep the incision clean and dry — no soaking in baths, pools, or hot tubs
- Use a log-rolling technique when getting in and out of bed
Early Recovery
Most patients can gradually increase their walking distance and duration during this period. Incision site soreness should continue to improve. Dr. Kazarian will see you for a follow-up visit to check your incision, review your progress, and adjust your activity level. Many patients are able to discontinue prescription pain medication within the first week and transition to over-the-counter options such as acetaminophen or ibuprofen.
- Continue to avoid bending, twisting, and lifting more than 5-10 pounds
- No strenuous exercise, running, or heavy housework
- Avoid prolonged sitting — take breaks to stand and walk every 30 minutes
- No driving until cleared by Dr. Kazarian (typically by week 2)
Gradual Return to Activity
During this phase, you will progressively resume more of your daily activities. Dr. Kazarian may refer you to physical therapy to begin a structured rehabilitation program focused on core strengthening, flexibility, and proper body mechanics. Light aerobic exercise such as walking and stationary cycling is usually permitted. Most patients who work in desk or office settings can return to work during this period, often around weeks 2 to 4.
- Follow your physical therapist's exercise program closely
- Avoid high-impact activities such as running, jumping, or contact sports
- Gradually increase lifting limits as directed by Dr. Kazarian
- Continue to use proper body mechanics when bending and lifting
Full Recovery and Return to Normal Activities
By six to twelve weeks, most patients have returned to their full range of activities, including work, exercise, and recreational pursuits. Dr. Kazarian will evaluate your progress and may clear you for more demanding physical activities and sports. Continued core strengthening and maintaining a healthy weight are important for long-term spine health and reducing the risk of future disc problems.
- Follow Dr. Kazarian's recommendations for returning to heavy lifting or high-impact sports
- Continue your home exercise program for ongoing spine health
- Report any new or recurring symptoms to Dr. Kazarian promptly
Follow-Up Schedule
- 1 to 2 weeks after surgery: Incision check, review of initial recovery progress, and adjustment of activity restrictions
- 4 to 6 weeks after surgery: Evaluation of nerve function recovery, discussion of physical therapy progression, and gradual return-to-work clearance
- 3 months after surgery: Comprehensive assessment of surgical outcome, nerve recovery, and clearance for full activities
- 6 to 12 months after surgery: Final follow-up to confirm long-term success and address any remaining concerns
When to Call Your Doctor
Contact our office immediately if you experience any of the following:
- New or worsening leg pain, numbness, or weakness after initial improvement
- Signs of infection at the incision site, including increasing redness, warmth, swelling, drainage, or fever above 101.5 degrees Fahrenheit
- Difficulty urinating, loss of bladder or bowel control, or new numbness in the groin or saddle area (seek emergency care immediately)
- Severe or worsening back pain that is not relieved by prescribed medications
- Sudden onset of leg weakness or difficulty walking that was not present before surgery
- Persistent nausea, vomiting, or inability to keep down fluids or medications
- Calf pain, swelling, or redness in one or both legs, which may indicate a blood clot

Take this info home
Scan this QR code with your phone to save this page and review it at home. You can also share it with family members.
https://kazarian-surgery-portal.vercel.app/en/surgeries/endoscopic-microdiscectomy
Questions about your Endoscopic Microdiscectomy/Laminectomy?
Ask below and we’ll do our best to help. For urgent concerns, please call our office directly.
Have a question about your upcoming surgery? Type it below and we’ll find the answer for you.