Dr. Erick Kazarian, MD
NYU Langone Spine Surgery — Patient Information
Scan the QR code to view this page online →

Anterior Cervical Discectomy and Fusion (ACDF)
Understanding Anterior Cervical Discectomy and Fusion
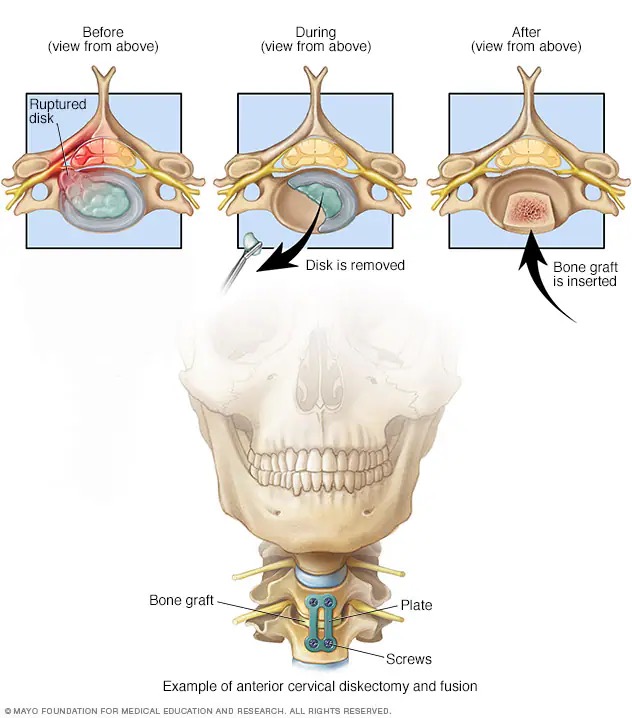
Anterior cervical discectomy and fusion, commonly known as ACDF, is a well-established surgical procedure used to relieve neck pain, arm pain, numbness, and weakness caused by a damaged or herniated disc in the cervical spine. During the procedure, Dr. Kazarian accesses the spine through a small incision in the front of your neck, removes the disc that is pressing on your spinal cord or nerve roots, and fuses the adjacent vertebrae together to restore stability. ACDF has been performed for decades and has an excellent track record of helping patients return to comfortable, active lives.
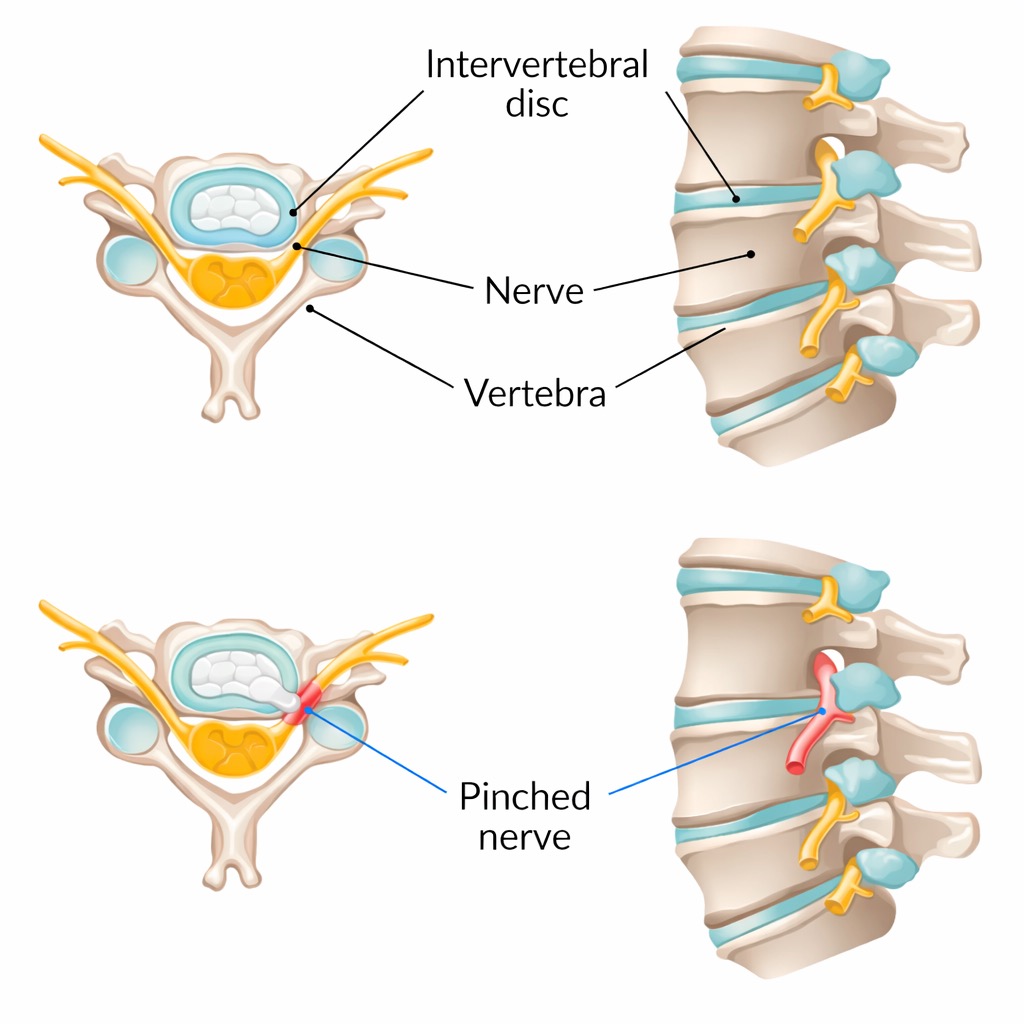
The cervical spine is made up of seven vertebrae that support your head and protect the spinal cord as it travels from your brain to the rest of your body. Between each vertebra sits a cushioning disc that acts as a shock absorber. Over time, or as a result of injury, these discs can bulge, herniate, or degenerate, putting pressure on nearby nerves. This pressure is what causes the pain, tingling, or weakness you may be experiencing in your neck, shoulders, arms, or hands. ACDF directly addresses the source of that pressure so your nerves can heal.
We understand that the idea of spine surgery can feel overwhelming, and we want you to know that you are in experienced, caring hands. Our surgical team will guide you through every step, from your first consultation through your full recovery. This page is designed to answer your questions, help you feel prepared, and give you a clear picture of what to expect before, during, and after your procedure. Please do not hesitate to reach out to our office if anything is unclear or if you need additional reassurance.
Images & Diagrams
Pre-Operative Instructions
Careful preparation before your surgery helps ensure the safest possible outcome and a smoother recovery. Please follow these instructions closely and contact our office with any questions.
Review all current medications and supplements with Dr. Kazarian.
1-2 weeks before surgeryStop blood thinners (warfarin, aspirin, Plavix), NSAIDs (ibuprofen, naproxen), and herbal supplements (fish oil, vitamin E, ginkgo) as directed. GLP-1 receptor agonists (Ozempic, Wegovy, Mounjaro, Trulicity, Saxenda) must be stopped 7 days before surgery due to the risk of aspiration under anesthesia. Do not stop any medication without Dr. Kazarian's approval.
Obtain medical clearance from your primary care physician and any relevant specialists.
2-4 weeks before surgeryThis may include blood work, an EKG, and a health review. Bring clearance letters and your CPAP machine (if applicable) on surgery day.
Do not eat or drink anything after midnight the night before surgery.
After midnight the night before surgeryThis includes water, coffee, gum, and mints. You may take approved medications with a small sip of water.
The NYU perioperative team will call you the day before surgery with your arrival time.
Day of surgeryLocation: NYU Langone Kimmel Pavilion, 424 East 34th Street, Manhattan. Bring a valid photo ID, insurance card, and medication list.
Arrange for a responsible adult to drive you home and stay with you for 24 hours.
Day of surgeryYou cannot drive after general anesthesia. Your driver should stay at the hospital during the procedure.
What to Expect on Surgery Day
ACDF is performed under general anesthesia and typically takes one to two hours. Most patients go home the same day or after one overnight stay. Here is a step-by-step overview of what your experience will look like.
Pre-Surgical Preparation
When you arrive at the hospital, you will check in and be taken to the pre-operative area. A nurse will verify your identity, review your medical history, and start an intravenous (IV) line. Dr. Kazarian and anesthesiologist will visit you to answer any final questions and confirm the surgical plan. The surgical site on your neck will be marked and gently cleaned. You may also receive a pre-operative medication to help you relax before being wheeled to the operating room.
Anesthesia
Once you are in the operating room, your anesthesiologist will administer general anesthesia through your IV line. You will fall asleep quickly and will not feel or remember any part of the surgery. A breathing tube will be gently placed to help you breathe during the procedure. Your vital signs, including heart rate, blood pressure, and oxygen levels, will be closely monitored throughout the entire operation to keep you safe and comfortable.
The Procedure
Dr. Kazarian makes a small incision, usually one to two inches, along a natural skin crease on the front of your neck. The muscles and soft tissues are gently moved aside to expose the cervical spine. Using fluoroscopic (X-ray) guidance, Dr. Kazarian identifies the damaged disc and carefully removes it, relieving the pressure on the spinal cord and nerve roots. The space left by the removed disc is then filled with a bone graft or a specially designed spacer to maintain proper disc height. A small metal plate and screws are placed on the front of the vertebrae to hold everything securely in position while the bones fuse together over the coming months.
Closing the Incision
After the graft and hardware are in place, Dr. Kazarian carefully repositions the soft tissues and muscles back to their natural positions. The incision is closed with dissolvable stitches or surgical adhesive strips, and a small sterile dressing is applied. In some cases, a small drain may be placed near the incision to prevent fluid buildup; this is typically removed before you are discharged. The incision is made along a natural neck crease, so the resulting scar is typically thin and becomes barely noticeable over time.
Recovery Room
You will be moved to the post-anesthesia recovery area, where nurses will closely monitor your breathing, blood pressure, pain levels, and neurological function as you wake up. You may feel some soreness in your throat and mild neck discomfort, which is normal. Once you are fully alert and can swallow comfortably, you will be offered ice chips and clear liquids. You will then be moved to your private room for an overnight stay, where your care team will continue to monitor your recovery. Most patients are discharged the following morning.
Risks & Potential Complications
As with any surgical procedure, ACDF carries certain risks. While serious complications are uncommon, it is important that you understand the potential risks so you can make a fully informed decision. Dr. Kazarian will discuss these with you in detail during your consultation.
Infection
Any time an incision is made, there is a small risk of infection at the surgical site. Infections are uncommon with cervical spine surgery and are typically treatable with antibiotics when caught early. Signs of infection include increasing redness, swelling, warmth, or drainage from the incision, as well as fever.
Blood Loss
Some bleeding is expected during surgery. Significant blood loss requiring a transfusion is rare in ACDF procedures, but your surgical team is prepared to manage this if needed.
Cerebrospinal Fluid (CSF) Leak
The spinal cord is surrounded by a protective membrane that contains cerebrospinal fluid. In rare cases, this membrane can be nicked during surgery, causing a fluid leak. If this occurs, it is typically repaired during the procedure and may require a short period of additional bed rest to allow it to heal.
Adjacent Segment Disease
After a spinal fusion, the vertebral levels immediately above or below the fused segment may experience increased stress over time. This can occasionally lead to disc degeneration or new symptoms at those neighboring levels months or years after surgery. Not all patients develop this, and it can often be managed conservatively if it does occur.
Neurologic Injury
Although rare, there is a risk of injury to the spinal cord or nerve roots during surgery. This could result in symptoms ranging from mild numbness or tingling in the arms or hands to, in very rare cases, more significant weakness or paralysis. Dr. Kazarian uses specialized techniques and monitoring to minimize this risk.
Hardware Failure
The metal plate and screws used to stabilize the fusion can, in rare cases, loosen, shift, or break before the bone has fully healed. If this occurs, a revision surgery may be needed to reposition or replace the hardware.
Non-Union (Pseudarthrosis)
Non-union means the bones do not fully fuse together as expected. This can result in continued pain or instability. Factors such as smoking, poor nutrition, and certain medical conditions can increase this risk. If non-union occurs, additional surgery may be necessary to achieve a solid fusion.
Difficulty Swallowing (Dysphagia)
Because the surgery is performed through the front of the neck, it is common to experience some difficulty or discomfort when swallowing in the days and weeks after surgery. This is usually temporary and resolves on its own, though in rare cases it may persist longer.
Voice Changes (Dysphonia)
Some patients notice hoarseness or subtle changes in their voice after surgery. This is caused by temporary irritation of the recurrent laryngeal nerve, which runs near the surgical area. In most cases, the voice returns to normal within a few weeks, though rarely the changes may be longer lasting.
Cervical Hematoma
A hematoma is a collection of blood that can form near the incision after surgery. In the neck, a significant hematoma can cause swelling that may affect breathing or swallowing. This is a rare but serious complication that your care team monitors for closely in the hours after surgery. If it occurs, it may require a return to the operating room to drain the blood collection.
Need for Further Surgery
While ACDF has a high success rate, there is a possibility that additional surgery may be needed in the future. This could be due to non-union, hardware issues, adjacent segment disease, or recurrence of symptoms. Dr. Kazarian will discuss the likelihood of this based on your individual circumstances.
Recovery
Recovery from ACDF surgery is a gradual process, but most patients begin to feel significant relief from their arm pain and neurological symptoms within the first few weeks. Full fusion of the vertebrae typically takes three to six months. Following Dr. Kazarian's post-operative guidelines, wearing your cervical collar as directed, and attending all follow-up appointments will give you the best chance at a successful, lasting outcome.
Prescribed Medications
| Medication | Type | Dosage | Frequency | When to Take |
|---|---|---|---|---|
| Flexeril (cyclobenzaprine) | Muscle Relaxer | 5 mg | Every 6 hours as needed | Take for moderate to severe muscle spasm or pain |
| Tylenol (acetaminophen) | Pain Reliever | 500–1000 mg | Every 6 hours as needed | Take for mild pain |
| Tramadol | Semi-Narcotic Pain Reliever | 75 mg | Every 6 hours as needed | Take for moderate to severe pain not controlled by Tylenol or NSAIDs |
Always take medications exactly as prescribed by your surgeon. Do not combine pain medications without consulting your doctor.
Early Recovery
It is normal to experience neck soreness, throat discomfort, mild difficulty swallowing, and some hoarseness during the first several days. These symptoms are caused by the surgical approach through the front of the neck and typically improve steadily. Arm pain and neurological symptoms such as tingling or numbness often improve quickly as the pressure on the nerves has been removed. Most patients transition from prescription pain medication to over-the-counter options within seven to ten days and can resume light daily activities such as simple meals and short walks.
- Wear your cervical collar as directed by Dr. Kazarian
- Do not lift anything heavier than 15 pounds
- Do not drive or operate machinery while taking narcotic pain medication
- Avoid bending, twisting, or rotating your neck
- Keep your incision clean and dry — do not submerge in water (no baths, pools, or hot tubs)
- Take short, gentle walks several times a day to promote circulation
Progressing Recovery
By two to six weeks, most patients notice a significant reduction in neck and arm pain and can comfortably perform many of their usual daily activities. Dr. Kazarian may clear you to begin driving and return to sedentary or light-duty work. Physical therapy may be introduced during this period to help restore neck range of motion, strengthen supporting muscles, and improve posture. Your cervical collar may be gradually weaned depending on your healing progress and Dr. Kazarian's assessment.
- Continue wearing your cervical collar if instructed by Dr. Kazarian
- Do not lift anything heavier than 15 pounds
- Follow your physical therapy program as prescribed
- No high-impact activities, contact sports, or vigorous exercise
- Continue to avoid excessive neck bending, twisting, or extension
Full Fusion and Return to Activity
The bone graft continues to mature and solidify during this period, and most patients achieve solid fusion by three to six months after surgery. Dr. Kazarian will order imaging studies such as X-rays to confirm that the fusion is progressing well. As the fusion solidifies, you will be able to gradually resume more physical activities. Most patients can return to full, unrestricted activity once their surgeon confirms a solid fusion. You should continue to practice good posture and body mechanics to protect your cervical spine long-term.
- Follow Dr. Kazarian's guidance on returning to strenuous activities and sports
- Report any new or recurring pain, numbness, or weakness promptly
- Attend all scheduled follow-up imaging and appointments
Follow-Up Schedule
- 2 weeks after surgery: Incision check, wound healing assessment, and review of early recovery progress
- 6 weeks after surgery: Clinical evaluation of pain and neurological function, possible X-rays, discussion of return to driving and light work
- 3 months after surgery: X-rays to assess fusion progress, physical therapy progress review, and gradual return to more activities
- 6 to 12 months after surgery: Follow-up imaging to confirm solid fusion and final assessment of outcomes
When to Call Your Doctor
Contact our office immediately if you experience any of the following:
- Increasing difficulty swallowing or breathing, or a feeling that your throat is swelling
- Sudden or worsening weakness, numbness, or tingling in your arms, hands, or legs
- Signs of infection at the incision site including increasing redness, warmth, swelling, drainage, or opening of the wound
- Fever of 101.5 degrees Fahrenheit (38.6 degrees Celsius) or higher
- Severe headache that does not respond to prescribed medication
- New onset of difficulty with balance or walking
- Significant increase in neck pain that is not controlled by your prescribed pain medication

Take this info home
Scan this QR code with your phone to save this page and review it at home. You can also share it with family members.
https://kazarian-surgery-portal.vercel.app/en/surgeries/acdf
Questions about your Anterior Cervical Discectomy and Fusion (ACDF)?
Ask below and we’ll do our best to help. For urgent concerns, please call our office directly.
Have a question about your upcoming surgery? Type it below and we’ll find the answer for you.