Dr. Erick Kazarian, MD
NYU Langone Spine Surgery — Patient Information
Scan the QR code to view this page online →

Anterior Lumbar Interbody Fusion (ALIF)
Anterior Lumbar Interbody Fusion (ALIF)
Anterior lumbar interbody fusion, commonly known as ALIF, is a two-stage spinal surgery that combines an anterior (front) approach through a small abdominal incision with posterior (back) robotic-guided percutaneous pedicle screw fixation. By approaching the spine from the front, Dr. Kazarian gains direct access to the intervertebral disc space without needing to disturb the back muscles, nerves, or spinal canal. Because the anterior portion of the procedure involves working near the major blood vessels in the abdomen, a vascular or general access surgeon assists during the approach to safely move these structures aside and create a clear path to the spine. The posterior screws are then placed through small incisions in the back using a state-of-the-art robotic navigation system for maximum precision.
ALIF offers several distinct advantages compared to a single posterior (back) approach to spinal fusion. The anterior approach allows Dr. Kazarian to place a larger interbody implant directly into the disc space, which provides a broader surface area for bone fusion and improved structural support. This larger implant also helps restore the natural curvature (lordosis) of the lumbar spine, which is essential for balanced posture and long-term spinal health. The posterior pedicle screws are placed percutaneously — meaning through tiny stab incisions — using a robotic arm that maps your spine in three dimensions and guides each screw along a pre-planned path with sub-millimeter accuracy. This combination of an anterior implant with robotic-assisted posterior fixation delivers the structural benefits of a 360-degree fusion while keeping tissue disruption to a minimum. ALIF is most commonly performed at the L4-L5 and L5-S1 levels of the lumbar spine, where the anterior approach provides excellent visualization and access.
Whether you are dealing with degenerative disc disease, spondylolisthesis, or a failed previous spinal surgery, ALIF may be a highly effective option for relieving pain and restoring spinal stability. Our surgical team, including both your spine surgeon and the vascular access surgeon, will work together to ensure the safest and most successful outcome. We are committed to guiding you through every phase of your care, from your initial consultation through your full recovery.
Images & Diagrams
Pre-Operative Instructions
Careful preparation before your anterior lumbar interbody fusion is essential for a safe procedure and a smooth recovery. Please follow these instructions closely, and contact our office with any questions.
Review all current medications and supplements with Dr. Kazarian.
2 weeks before surgeryStop blood thinners (warfarin, aspirin, Plavix), NSAIDs (ibuprofen, naproxen), and herbal supplements (fish oil, vitamin E, ginkgo) as directed. GLP-1 receptor agonists (Ozempic, Wegovy, Mounjaro, Trulicity, Saxenda) must be stopped 7 days before surgery due to the risk of aspiration under anesthesia. Do not stop any medication without Dr. Kazarian's approval.
Obtain medical clearance from your primary care physician and any relevant specialists.
2-4 weeks before surgeryThis may include blood work, an EKG, and a health review. Bring clearance letters and your CPAP machine (if applicable) on surgery day.
Follow the bowel preparation instructions provided by Dr. Kazarian's office.
1 day before surgeryThis may include a clear liquid diet, a gentle laxative, or specific dietary changes the day before surgery. A clean bowel allows safer abdominal access.
Do not eat or drink anything after midnight the night before surgery.
After midnight the night before surgeryThis includes water, coffee, gum, and mints. You may take approved medications with a small sip of water.
The NYU perioperative team will call you the day before surgery with your arrival time.
Day of surgeryLocation: NYU Langone Kimmel Pavilion, 424 East 34th Street, Manhattan. Bring a valid photo ID, insurance card, and medication list.
Arrange for a responsible adult to drive you home and stay with you for 24-48 hours.
Arrange before surgery dayYou cannot drive after general anesthesia. Your driver should stay at the hospital during the procedure.
What to Expect on Surgery Day
Knowing what to expect before, during, and after your anterior lumbar interbody fusion can help ease any anxiety and allow you to feel confident and prepared. Here is an overview of your surgical experience, step by step.
Check-In and Pre-Operative Preparation
You will arrive at the hospital approximately two hours before your scheduled surgery time. Our nursing team will verify your identity, review your medical history, and confirm the surgical level with your spine surgeon. An IV line will be placed, and you will change into a hospital gown. Both your spine surgeon and the vascular access surgeon will visit you to review the procedure and answer any remaining questions. Your anesthesiologist will also discuss the anesthesia plan and any concerns you may have.
Anesthesia and Positioning
ALIF is performed under general anesthesia, so you will be completely asleep and feel no pain during the procedure. Once anesthesia is administered, you will be carefully positioned lying flat on your back (supine position) on the operating table. Your abdomen will be cleaned and draped in a sterile manner. The supine position allows the surgical team to access the spine through the front of the body, and your care team will ensure all pressure points are properly padded for your comfort and safety.
Abdominal Approach and Vascular Mobilization
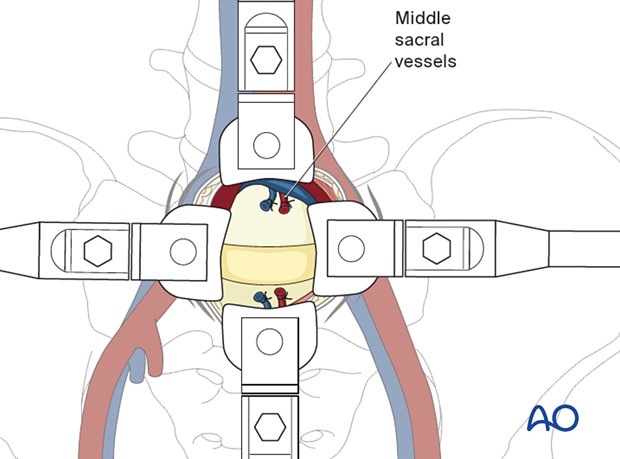
The vascular or general access surgeon will begin by making an incision in your lower abdomen, typically three to five inches in length. The abdominal muscles are gently separated rather than cut, and the peritoneum (the lining of the abdominal cavity) is carefully moved aside. The access surgeon then identifies and gently retracts the major blood vessels, including the aorta and vena cava or the iliac vessels, to create a safe corridor directly to the front of the spine. This collaborative approach ensures that these critical structures are protected throughout the procedure.
Disc Removal and Implant Placement
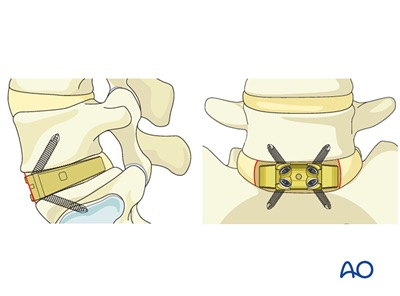
With the spine now fully visible, Dr. Kazarian removes the damaged or degenerated disc material from between the vertebrae. The disc space is carefully prepared and measured, and a precisely sized interbody implant (often made of PEEK, titanium, or bone allograft) is placed into the space. The implant is packed with bone graft material to promote fusion. The direct anterior view allows Dr. Kazarian to position the implant optimally, restoring the proper height and curvature of the lumbar spine. Once the implant is securely in place, the vascular surgeon allows the blood vessels to return to their natural position and the abdominal incision is closed.
Robotic-Guided Posterior Pedicle Screw Placement
After the anterior stage is complete, you will be repositioned and Dr. Kazarian will place posterior percutaneous pedicle screws through small incisions in your back. This is where the procedure takes advantage of cutting-edge robotic technology: a robotic arm, guided by a three-dimensional CT-based navigation system, maps your unique spinal anatomy in real time and guides each screw along a pre-planned trajectory with remarkable precision. The robotic system allows for sub-millimeter accuracy in screw placement, which means smaller incisions, less time in the operating room, and greater confidence that every screw is in the ideal position. The screws and connecting rods lock the treated segment in place and provide the stability needed for the bone graft to fuse solidly over the coming months.
Closing the Posterior Incisions
After all posterior screws and rods are in place and final imaging confirms proper alignment, the small posterior incisions are closed with dissolvable sutures and covered with sterile dressings. In some cases, a small drain may be placed near one of the incision sites to prevent fluid buildup; this is typically removed before you are discharged.
Recovery Room
You will be transferred to the post-anesthesia recovery area, where nurses will closely monitor your vital signs, pain levels, circulation in your legs, and abdominal function. You will then be moved to your private room, where your care team will continue to monitor your recovery. A physical therapist will help you safely sit, stand, and walk during your hospital stay. Most patients are discharged one to three days after surgery.
Risks & Potential Complications
All surgical procedures carry some degree of risk. Dr. Kazarian takes every precaution to minimize these risks, and serious complications are uncommon. Understanding the potential risks helps you make an informed decision and know what to watch for during your recovery.
Infection
There is a small risk of infection at the surgical site or deeper around the spine. Antibiotics are given before and after surgery to reduce this risk. Signs of infection include increasing redness, swelling, warmth, or drainage from the incision, as well as fever.
Blood Loss
Some blood loss is expected during spinal fusion surgery. In rare cases, significant blood loss may occur that requires a blood transfusion. Your surgical team monitors blood loss closely throughout the procedure.
Cerebrospinal Fluid Leak
The protective membrane (dura) surrounding the spinal cord and nerves may occasionally be opened during surgery, allowing spinal fluid to leak. If this occurs, it is typically repaired during the procedure. In rare cases, additional treatment may be needed after surgery.
Adjacent Segment Disease
After fusion, the spinal segments above and below the fused area may experience increased stress over time. This can lead to degeneration at those neighboring levels, potentially causing new symptoms months or years after surgery. Not everyone who has a fusion develops this condition.
Neurologic Injury
There is a small risk of injury to the spinal nerves during surgery, which could result in new or worsened numbness, tingling, weakness, or pain in the legs. In very rare cases, more significant nerve injury may occur. Dr. Kazarian uses specialized techniques and monitoring to minimize this risk.
Hardware Failure
The interbody implant, posterior pedicle screws, rods, or other hardware used to stabilize the spine can occasionally loosen, shift, or break before the fusion has fully healed. The precision of robotic-guided screw placement helps minimize this risk by ensuring optimal screw positioning, but if hardware complications do occur, additional surgery may be needed to replace or adjust the affected components.
Nonunion (Pseudarthrosis)
In some cases, the bone may not fully fuse as expected, a condition called nonunion or pseudarthrosis. This can cause persistent or recurring pain and instability. Factors such as smoking, diabetes, and poor nutrition can increase this risk. If nonunion occurs, a revision surgery may be recommended.
Need for Additional Surgeries
While spinal fusion is often successful, there is a possibility that additional surgeries may be needed in the future. This could be due to nonunion, hardware issues, adjacent segment disease, or other factors. Dr. Kazarian will discuss your individual risk factors with you.
Retrograde Ejaculation
In male patients, the anterior approach passes near nerves that control ejaculatory function. There is a small risk that these nerves may be affected, which can cause semen to travel backward into the bladder instead of forward during ejaculation. This does not affect the ability to achieve an erection or orgasm, but it can impact fertility. Dr. Kazarian will discuss this risk with you in detail.
Major Vascular Injury
The anterior approach requires working near the large blood vessels (aorta and vena cava) in front of the spine. While rare, there is a risk of injury to these vessels during surgery. A vascular surgeon is often present or available during the procedure to help manage this risk and ensure the safest possible approach.
Recovery
Recovery from anterior lumbar interbody fusion with robotic-guided posterior pedicle screws is a gradual process that unfolds over several months. Because the anterior portion is performed through the abdomen, you may experience some abdominal soreness and temporary changes in bowel function during the early days. The posterior screw incisions are small and typically cause only mild tenderness. Most patients notice significant improvement in their leg and back pain within the first few weeks. The bone fusion process takes approximately six to twelve months, during which time you will gradually increase your activity level under the guidance of your surgical team. Our goal is to help you return to a comfortable, active life with a stable and well-aligned spine.
Prescribed Medications
| Medication | Type | Dosage | Frequency | When to Take |
|---|---|---|---|---|
| Flexeril (cyclobenzaprine) | Muscle Relaxer | 5 mg | Every 6 hours as needed | Take for moderate to severe muscle spasm or pain |
| Tylenol (acetaminophen) | Pain Reliever | 500–1000 mg | Every 6 hours as needed | Take for mild pain |
| Oxycodone | Opiate Pain Reliever | 5–10 mg | Every 4–6 hours as needed | Take for moderate to severe pain not controlled by Tylenol or NSAIDs |
Always take medications exactly as prescribed by your surgeon. Do not combine pain medications without consulting your doctor.
Early Hospital and Home Recovery
You will spend one to three nights in the hospital, where the team will monitor your pain, circulation, and return of bowel function. Walking short distances with assistance typically begins the day after surgery and is essential for promoting healing and preventing blood clots. Once home, focus on rest, gentle walking, and allowing both the abdominal incision and the small posterior screw incisions to heal. You may experience mild abdominal bloating or changes in appetite as your digestive system returns to normal, along with mild tenderness at the posterior incision sites.
- No bending, lifting, or twisting (BLT precautions)
- Do not lift anything heavier than 5 pounds
- No driving while taking opioid pain medications
- Avoid prolonged sitting for more than 20 to 30 minutes at a time
- No soaking the incision in water (no baths, pools, or hot tubs)
Gradual Activity Increase
Most patients begin to feel noticeably better during this period, with decreasing abdominal and back discomfort. You will gradually increase your walking distance and duration each week. Dr. Kazarian may clear you to begin driving once you are off opioid medications and can safely turn to check blind spots, typically around three to four weeks. Light daily activities such as cooking and self-care become more manageable. Your incision should be well healed by the end of this phase.
- Continue to avoid lifting more than 10 pounds
- No vigorous exercise, running, or high-impact activities
- Avoid prolonged sitting beyond 30 to 45 minutes without a break
- Continue BLT (bend, lift, twist) precautions as directed
Physical Therapy and Strengthening
Dr. Kazarian will likely recommend beginning a structured physical therapy program around the six-week mark. Physical therapy will focus on core stabilization, gentle lumbar flexibility, and gradually rebuilding strength in the muscles that support your spine. Many patients return to desk-based or light-duty work during this period, depending on the physical demands of their job. Imaging may be performed to assess early signs of bone fusion.
- Avoid heavy lifting over 15 to 20 pounds until cleared
- No contact sports or high-impact activities
- Follow your physical therapist's exercise progression carefully
Fusion Maturation and Full Recovery
By three to six months, the bone graft within the interbody implant is expected to mature and solidify into a solid fusion. Dr. Kazarian will evaluate the fusion progress with follow-up imaging. As the fusion becomes solid, you will be able to return to most normal activities, including more strenuous physical tasks and recreational exercise. Patients with physically demanding jobs may be cleared to return to full duty during this period. Most patients report substantial or complete relief from their preoperative leg and back pain by this stage.
- Follow Dr. Kazarian's clearance for return to full activities
- Continue core strengthening and good body mechanics long-term
Follow-Up Schedule
- 2 weeks after surgery: Incision check, wound healing assessment, and review of early recovery progress
- 6 weeks after surgery: Clinical evaluation of pain and neurological function, possible X-rays, discussion of return to driving and light work
- 3 months after surgery: X-rays to assess fusion progress, physical therapy progress review, and gradual return to more activities
- 6 to 12 months after surgery: Follow-up imaging to confirm solid fusion and final assessment of outcomes
When to Call Your Doctor
Contact our office immediately if you experience any of the following:
- Fever of 101.5 degrees Fahrenheit (38.6 degrees Celsius) or higher, which may indicate infection
- Increasing redness, swelling, warmth, or drainage from the abdominal incision
- Severe or worsening abdominal pain, significant bloating, inability to pass gas, or persistent nausea and vomiting, which may indicate ileus (temporary bowel paralysis) or other abdominal complications
- New or worsening leg pain, numbness, tingling, or weakness that was not present before surgery
- Signs of vascular complications, including sudden leg swelling, coldness, discoloration, or loss of pulse in one or both legs
- Difficulty urinating, inability to empty your bladder, or loss of bowel or bladder control
- Sudden onset of chest pain, shortness of breath, or calf swelling and tenderness, which may indicate a blood clot
- Severe or uncontrolled pain that is not adequately managed by your prescribed medications

Take this info home
Scan this QR code with your phone to save this page and review it at home. You can also share it with family members.
https://kazarian-surgery-portal.vercel.app/en/surgeries/anterior-lumbar-interbody-fusion
Questions about your Anterior Lumbar Interbody Fusion (ALIF)?
Ask below and we’ll do our best to help. For urgent concerns, please call our office directly.
Have a question about your upcoming surgery? Type it below and we’ll find the answer for you.